How Hospitals Deploy On-Premise Clinical AI Assistants
Date
January 28th, 2026
Reading Time
7 mins
Abstract
As hospitals move beyond experimental pilots, architectural priorities shift from isolated models toward intelligent systems that actively support decisions within real clinical and operational workflows. In healthcare environments where patient safety, regulatory accountability, and data sovereignty are strict requirements rather than preferences, deploying these systems inside hospital owned infrastructure remains the dominant approach for clinical assistants that must operate under controlled governance frameworks.
This article examines how hospitals design on premise clinical assistants as integrated decision systems that combine predictive analytics, large language model reasoning, and autonomous orchestration layers. Rather than treating intelligence as a standalone capability, clinical assistance is framed as an operational system that consumes governed clinical data, executes inference locally, and augments human decision making through deterministic and auditable behavior. The discussion focuses on system architecture, data ingestion pipelines, security and access controls, and lifecycle management practices required to operate such systems reliably within hospital environments.
1. Why On-Premise Clinical AI Still Matters in Hospitals
Hospitals increasingly require intelligent systems that operate within strictly defined trust boundaries. While cloud platforms are effective for rapid prototyping and exploratory analytics, deploying decision support capabilities inside hospital owned infrastructure remains essential when patient data sensitivity, regulatory compliance, and predictable system behavior take priority over elasticity or deployment speed. In clinical environments, uncertainty in data handling or execution behavior is not an acceptable tradeoff for convenience.
Clinical assistants deployed on premises allow hospitals to maintain complete control over data residency, inference execution, and decision logic. Protected health information remains confined to internal networks governed by existing security controls, while inference workloads execute locally without reliance on external application programming interfaces or variable network conditions. This architecture is especially critical for time sensitive clinical and operational scenarios where latency, availability, and deterministic responses directly influence patient outcomes and clinician trust.
In practice, on premises deployment is not positioned as a replacement for cloud infrastructure. Instead, it functions as the execution layer for high risk and mission critical workloads, while cloud environments support model training, large scale analytics, experimentation, and non clinical use cases. This hybrid operating model enables hospitals to scale intelligent automation responsibly by separating exploratory innovation from regulated clinical execution, while preserving governance, auditability, and organizational accountability.
2. Core Use Cases for On-Prem Clinical AI Assistants
On premise clinical AI assistants are deployed at points where contextual sensitivity, operational frequency, and clinical or operational risk intersect. These systems are not designed as open conversational interfaces. Instead, they are purpose built assistants embedded directly into clearly defined clinical and administrative workflows, where inputs, outputs, and runtime behavior are tightly scoped and governed.
In clinical documentation workflows, AI assistants apply large language model based understanding to transform unstructured clinician input into structured medical records. Common functions include organizing progress notes, summarizing patient encounters, and drafting discharge documentation. Crucially, these systems emphasize extraction, summarization, and normalization rather than free form generation. Outputs are constrained by predefined templates, clinical vocabularies, and validation rules to prevent the introduction of unsupported diagnoses, treatment suggestions, or speculative conclusions that could compromise patient safety.
Clinical decision support scenarios rely primarily on predictive analytics rather than generative reasoning. Models are trained to estimate early deterioration signals, readmission risk, length of stay, and resource utilization patterns using historical and near real time hospital data. The assistant surfaces these signals contextually within existing clinical systems such as electronic health records, accompanied by feature level explanations or trend summaries. It does not issue prescriptive decisions. Instead, it augments clinician judgment by reducing cognitive load and accelerating pattern recognition.
Within hospital operations, on premise AI assistants support staffing forecasts, bed capacity management, operating room scheduling, and throughput optimization. These systems continuously analyze live operational data streams including admissions, transfers, discharges, staffing rosters, and equipment availability. Predictive outputs are refreshed at high frequency and integrated into operational dashboards, enabling administrators to anticipate constraints before they materialize rather than responding to disruptions after the fact.
Across all use cases, clinical AI assistants function as decision accelerators rather than decision makers. System behavior is bounded by confidence thresholds, alerting logic, and escalation rules defined during deployment. When uncertainty exceeds acceptable limits, the system defers to human review rather than emitting low confidence outputs. This design ensures that accountability for clinical and operational decisions remains firmly with clinicians and administrators, while AI contributes speed, consistency, and analytical depth.
3. Reference Architecture: On-Prem Clinical AI Assistant
A production grade on premise clinical AI assistant is implemented as a layered system that integrates governed data pipelines, local inference capabilities, and workflow orchestration logic. The design emphasizes determinism, observability, and control, ensuring that AI behavior remains predictable and auditable within hospital infrastructure.
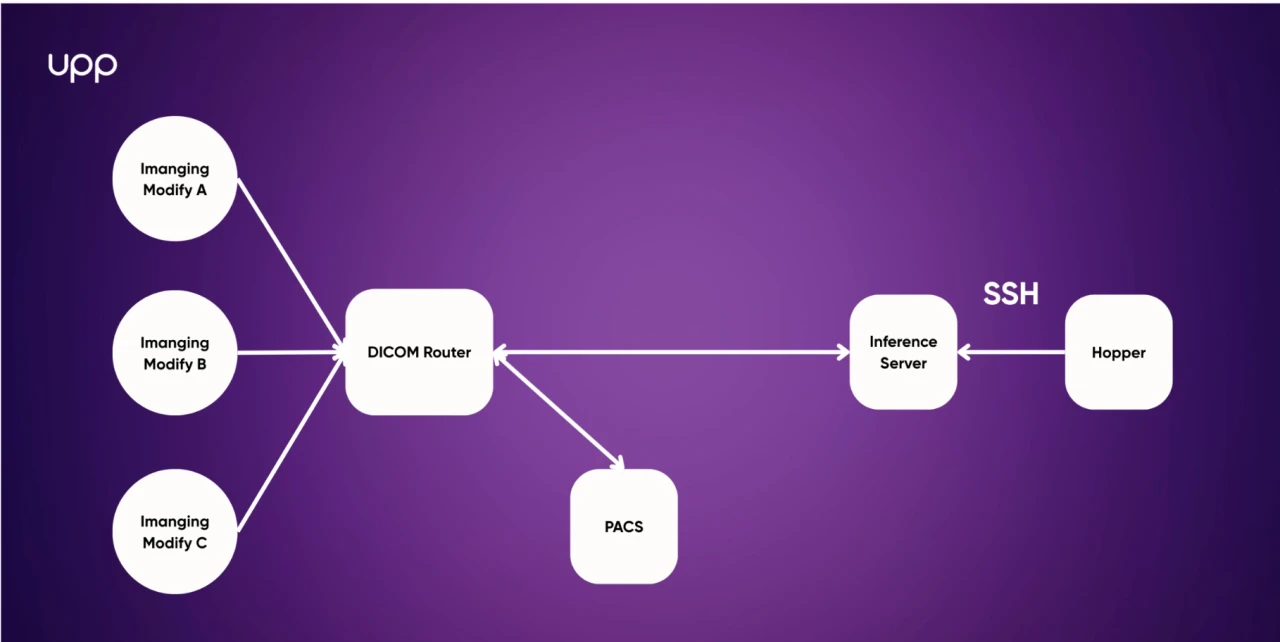
At the ingestion layer, data flows from electronic health records, laboratory systems, imaging platforms, medical devices, and administrative applications using healthcare interoperability standards such as HL7, FHIR, and DICOM. Event driven ingestion pipelines validate, normalize, and enrich incoming data before it is persisted, allowing near real time signal availability while enforcing data quality constraints and schema consistency. This layer acts as the primary control point for data contracts between source systems and downstream intelligence components.
The clinical data layer is commonly implemented using an on premise lakehouse architecture that separates raw data, curated clinical datasets, and feature ready representations. This separation enables longitudinal patient views, reproducible feature engineering, and controlled reuse of clinical signals across multiple models and agents. Lineage tracking, access control, and audit trails are built into this layer to support regulatory compliance and retrospective analysis.
Above the data layer, the AI stack hosts multiple forms of intelligence with clearly defined responsibilities. Predictive models produce structured outputs such as risk scores, forecasts, and classification signals derived from engineered features. Large language model components focus on contextual understanding of unstructured inputs, including clinical notes, protocols, and guidelines. An orchestration layer coordinates these components by applying decision policies, confidence thresholds, and routing logic that determine how outputs are surfaced within clinical and operational workflows.
Inference is executed locally using containerized services orchestrated by platforms such as Kubernetes or equivalent cluster managers. This deployment model allows hospitals to scale inference workloads, manage versioned model rollouts, and isolate failures without relying on external services or network connectivity. Local execution ensures predictable latency and supports high availability requirements for time sensitive clinical scenarios.
Security and compliance controls span all layers of the system. Role based and context aware access controls govern who can access data, models, and decision outputs. Data is encrypted at rest and in transit, and immutable audit logs capture every access and inference event. By operating entirely on premise, hospitals retain full ownership of the AI trust boundary, ensuring that sensitive clinical data, decision logic, and system behavior remain under institutional control.
4. From Raw Clinical Data to Intelligent Decisions
The defining capability of modern clinical AI assistants is not model scale, but decision orchestration. Raw clinical data is continuously transformed into structured, policy compliant signals that intelligent agents can interpret and act upon within defined clinical and operational contexts.
Predictive analytics identifies patterns across patient flow, equipment utilization, staffing demand, and clinical risk indicators. In parallel, large language model reasoning components interpret unstructured inputs such as clinical notes, care guidelines, and institutional policies, converting free text into contextual explanations that align with clinical intent. Autonomous agents sit above these intelligence layers, combining quantitative signals and contextual understanding to prioritize actions, optimize workflows, and surface time sensitive alerts to clinicians and administrators.
Critically, these systems are not designed to operate without supervision. Decision thresholds, escalation rules, clinician review checkpoints, and explainability constraints are embedded directly into the orchestration layer. Every recommendation or alert is produced within predefined confidence boundaries and traceable logic paths, ensuring that AI systems support clinical judgment rather than replace it. Accountability remains with human decision makers, while AI accelerates access to relevant insights at the moment they are needed most.
5. MLOps and Lifecycle Management in Hospitals
Hospitals manage intelligent clinical systems with the same rigor applied to other regulated healthcare technologies. Models and orchestration logic are versioned, validated offline, and approved through formal governance processes before entering production environments.
Once deployed, clinical assistants are monitored continuously against defined clinical and operational KPIs. Feedback loops capture incorrect predictions, workflow friction, and user trust signals. These inputs drive refinements to data pipelines, feature engineering, and decision policies, rather than uncontrolled or ad hoc model retraining.
Learning occurs primarily at the system level, prioritizing stability, traceability, and regulatory compliance over rapid or experimental iteration.
6. On-Premise Versus Hybrid AI Deployment
Most mature healthcare organizations adopt a hybrid deployment model. On premise systems are responsible for sensitive inference, clinical decision support, and workflow automation, while cloud environments are used for experimentation, advanced analytics, and non clinical automation.
This separation allows hospitals to scale innovation without weakening governance or accountability. On premise AI remains the operational core of clinical systems, executing decisions and automation within controlled trust boundaries. Cloud platforms extend analytical and development capabilities in areas where data sensitivity is lower and risk tolerance is higher, enabling faster iteration without compromising clinical safety.
7. Conclusion
Deploying on-premise clinical assistants reflects a broader shift toward intelligent systems built for clinical reality. Success depends less on model novelty and more on disciplined architecture, governed data pipelines, and robust operational controls.
Hospitals that succeed treat these systems as integrated components of clinical and operational workflows, constrained by safety requirements and clear accountability. In this model, intelligent automation augments human decision making by transforming data into timely, contextual insight, delivered securely, predictably, and responsibly.
Tags cloud
Newsletter
DISCOVER MORE































































![[Recap] UPP Global Technology JSC Establishing Anniversary](/homepage/news-section/new-4.webp)






































LET’S TALK...
Content delivered to your inbox






ENTER YOUR EMAIL
YOU WANT TO...



Hanoi, Vietnam
Web3 Tower, No. 15, Alley 4, Duy Tan, Cau Giay, Hanoi, Vietnam